Abstract
Increased longevity and population aging will increase the number of men with late onset hypogonadism. It is a common condition, but often underdiagnosed and undertreated. The indication of testosterone-replacement therapy (TRT) treatment requires the presence of low testosterone level, and symptoms and signs of hypogonadism. Although controversy remains regarding indications for testosterone supplementation in aging men due to lack of large-scale, long-term studies assessing the benefits and risks of testosterone-replacement therapy in men, reports indicate that TRT may produce a wide range of benefits for men with hypogonadism that include improvement in libido and sexual function, bone density, muscle mass, body composition, mood, erythropoiesis, cognition, quality of life and cardiovascular disease. Perhaps the most controversial area is the issue of risk, especially possible stimulation of prostate cancer by testosterone, even though no evidence to support this risk exists. Other possible risks include worsening symptoms of benign prostatic hypertrophy, liver toxicity, hyperviscosity, erythrocytosis, worsening untreated sleep apnea or severe heart failure. Despite this controversy, testosterone supplementation in the United States has increased substantially over the past several years. The physician should discuss with the patient the potential benefits and risks of TRT. The purpose of this review is to discuss what is known and not known regarding the benefits and risks of TRT.
Keywords: hypogonadism, testosterone replacement therapy, erectile dysfunction, osteoporosis, cardiovascular disease
Hypogonadism is a clinical condition in which low levels of serum testosterone are found in association with specific signs and symptoms. When hypogonadism occurs in an older man, the condition is often called andropause or androgen deficiency of the aging male or late onset hypogonadism (LOH).1 The most easily recognized clinical signs of relative androgen deficiency in older men are a decrease in muscle mass and strength, a decrease in bone mass and osteoporosis, and an increase in central body fat. However, symptoms such as a decrease in libido and sexual desire, forgetfulness, loss of memory, anemia, difficulty in concentration, insomnia, and a decreased sense of well-being are more difficult to measure and differentiate from hormone-independent aging. This condition may result in significant detriment to quality of life and adversely affect the function of multiple organ systems.13 A health factor-independent, age-related longitudinal decrease in serum testosterone levels has been reported.4 This LOH is important since it features many potentially serious consequences that can be readily avoided or treated, and the affected sector of the population is currently expanding in number. Prospective population-based studies reported in the past decade indicate that low testosterone levels are associated with an increase in the risk for developing type 2 diabetes mellitus and metabolic syndrome and possibly a reduction in survival. Results were similar for bioavailable testosterone.57 In men, endogenous testosterone concentrations are inversely related to mortality due to cardiovascular disease and all causes. Low testosterone may be a predictive marker for those at high risk of cardiovascular disease.8 Also, low testosterone levels were associated with increased mortality in male veterans9 but this association could not be confirmed in the Massachusetts Male Aging Study10 or the New Mexico Aging Study.11
As the clinical symptoms of hormone deficiency in older males may be nonspecific, and since a substantial number of relatively asymptomatic elderly men have testosterone levels outside the normal range for young adults, investigators have suggested that testosterone replacement therapy is only warranted in the presence of both clinical symptoms suggestive of hormone deficiency and decreased hormone levels.12 Restoring serum testosterone levels to the normal range using testosterone replacement therapy results in clinical benefits in some of these areas. Successful management of testosterone replacement therapy requires appropriate evaluation and an understanding of the benefits and risks of treatment.
Due to the baby boom that occurred after World War II, the percentage of population in the older age group in developed countries is increasing. Testosterone deficiency is a common disorder in middle-aged and older men but it is underdiagnosed and often untreated. Clinicians tend to overlook it, and the complaints of androgen-deficient men are merely considered part of aging. Hypogonadism affects an estimated 2 million to 4 million men in the United States. Many patients can derive significant benefits from treatment. Testosterone supplementation in the United States has increased substantially over the past several years.13 However, it has been estimated that only 5% of affected men currently receive treatment.
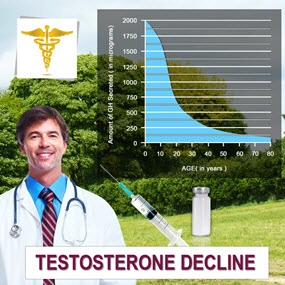
The decline of serum testosterone levels appears to be a gradual, age-related process resulting in an approximate 1% annual decline after age 30. In cross-sectional and longitudinal studies of men aged 30 or 40 years and above, total, bioavailable and free testosterone concentrations fall with increasing age with a steeper decline in bioavailable and free compared with total testosterone concentrations.4,14,15 In older men above the age of 65 or 70 years, the changes in total testosterone are overshadowed by a more significant decline in free testosterone levels.16,17 This is a consequence of the age-associated increase of the levels of sex hormone binding globulin (SHBG) demonstrated by cross-sectional studies, and has now been confirmed by longitudinal studies.18,19 Although the fall is gradual, by the eighth decade, according to the Baltimore Longitudinal Study, 30% of men had total testosterone values in the hypogonadal range, and 50% had low free testosterone values. The rate of age-related decline in serum testosterone levels varies in different individuals and is affected by chronic disease and medications.20 There is evidence that many of these men are not symptomatic.21
Multiple mechanisms are likely to influence the decline in testosterone levels in aging men.22 Lower testosterone levels may result from reduced testicular responses to gonadotrophin stimuli with aging, coupled with incomplete hypothalamopituitary compensation for the fall in total and free testosterone levels.23,24 Whether the age-dependent decline in androgen levels leads to health problems in older men is being debated vigorously.21,25
At present, the diagnosis of hypogonadism requires the presence of symptoms and signs suggestive of testosterone deficiency.1,26 The symptom most associated with hypogonadism is low libido.2729 Other manifestations of hypogonadism include erectile dysfunction, decreased muscle mass and strength, increased body fat, decreased bone mineral density and osteoporosis, mild anemia, breast discomfort and gynecomastia, hot flushes, sleep disturbance, body hair and skin alterations, decreased vitality, and decreased intellectual capacity (poor concentration, depression, fatigue).30 The problem is many of the symptoms of late life hypogonadism are similar in other conditions31,32 or are physiologically associated with the aging process.33 One or more of these symptoms must be corroborated with a low serum testosterone level.21,25,34 Depression, hypothyroidism and chronic alcoholism should be excluded, as should the use of medications such as corticosteroids, cimetidine, spironolactone, digoxin, opioid analgesics, antidepressants and antifungal drugs. Of course, diagnosis of LOH should never be undertaken during an acute illness, which is likely to result in temporarily low testosterone levels ().
Approach to the diagnosis and treatment of late onset hypogonadism (ADAM = St. Louis University Androgen Deficiency in Aging Males Questionnaire).
See the original post:
The benefits and risks of testosterone replacement therapy: a ...
Contact Us Today For A Free Consultation

- 0001) Part 2: Effect of Testosterone Replacement Therapy on Prostate Tissue in Men with Late-Onset Hypogonadism (Dramatic Health) [Last Updated On: March 24th, 2018] [Originally Added On: May 7th, 2011]
- 0002) Full: Effect of Testosterone Replacement Therapy on Prostate Tissue in Men with Late-Onset Hypogonadism (Dramatic Health) [Last Updated On: May 3rd, 2023] [Originally Added On: May 7th, 2011]
- 0003) Testosterone Replacement Therapy (TRT): Optimizing Clinical Outcomes - Michael Aziz, MD [Last Updated On: November 12th, 2023] [Originally Added On: May 8th, 2011]
- 0004) Part 1: Effect of Testosterone Replacement Therapy on Prostate Tissue in Men with Late-Onset Hypogonadism (Dramatic Health) [Last Updated On: March 24th, 2018] [Originally Added On: May 8th, 2011]
- 0005) Part 4: Effect of Testosterone Replacement Therapy on Prostate Tissue in Men with Late-Onset Hypogonadism (Dramatic Health) [Last Updated On: November 12th, 2023] [Originally Added On: May 30th, 2011]
- 0006) Part 3: Effect of Testosterone Replacement Therapy on Prostate Tissue in Men with Late-Onset Hypogonadism (Dramatic Health) [Last Updated On: November 15th, 2023] [Originally Added On: June 2nd, 2011]
- 0007) Testosterone Replacement [Last Updated On: November 23rd, 2023] [Originally Added On: June 7th, 2011]
- 0008) Medical Professor on Testosterone Replacement Therapy [Last Updated On: November 17th, 2023] [Originally Added On: June 14th, 2011]
- 0009) Sean McCorkle Discusses Testosterone Replacement Therapy [Last Updated On: November 18th, 2023] [Originally Added On: July 11th, 2011]
- 0010) Use of Testosterone in Men With Prostate Cancer [Last Updated On: November 22nd, 2023] [Originally Added On: September 28th, 2011]
- 0011) Low Testosterone (Low T) - Video [Last Updated On: November 25th, 2024] [Originally Added On: December 10th, 2011]
- 0012) Transdermal Drug Delivery - Technologies, Markets, and Companies [Last Updated On: April 29th, 2025] [Originally Added On: February 2nd, 2012]
- 0013) How Testosterone Replacement Therapy Builds Muscle and Stops Pain [Last Updated On: February 4th, 2024] [Originally Added On: February 4th, 2012]
- 0014) Teva, BioSante’s Testosterone Gel for Men Wins Approval From U.S. FDA [Last Updated On: January 11th, 2018] [Originally Added On: February 15th, 2012]
- 0015) FDA approves Teva, BioSante testosterone gel [Last Updated On: January 18th, 2018] [Originally Added On: February 15th, 2012]
- 0016) Teva Fourth-Quarter Profit Rises on Cephalon Purchase [Last Updated On: January 16th, 2018] [Originally Added On: February 15th, 2012]
- 0017) Renowned Dr. Oz and the Acclaimed Financial Times Now Have Featured Dr. Lionel Bisson, Founder of ... [Last Updated On: April 27th, 2025] [Originally Added On: February 17th, 2012]
- 0018) Omaha man says testosterone replacement therapy changed his life [Last Updated On: March 7th, 2026] [Originally Added On: May 5th, 2012]
- 0019) Auxilium Pharmaceuticals, Inc. and GlaxoSmithKline LLC Enter Into a Co-Promotion Agreement for Testim® in the U.S. [Last Updated On: May 6th, 2025] [Originally Added On: May 21st, 2012]
- 0020) Hormone therapy results in weight loss [Last Updated On: January 27th, 2018] [Originally Added On: June 25th, 2012]
- 0021) Testosterone in Women-Putting Your Sex Drive Bacl On Track - Video [Last Updated On: December 31st, 2024] [Originally Added On: November 2nd, 2012]
- 0022) Men's Health PITCH: Testosterone - Video [Last Updated On: January 1st, 2025] [Originally Added On: November 2nd, 2012]
- 0023) Dr. Karron Power Appears on Nightline - Testosterone Therapy - Video [Last Updated On: January 1st, 2025] [Originally Added On: November 2nd, 2012]
- 0024) Testosterone Replacement Therapy: Who is TRT Best For? - Video [Last Updated On: January 2nd, 2025] [Originally Added On: November 2nd, 2012]
- 0025) Female sex-enhancing nasal spray undergoing clinical trials [Last Updated On: November 19th, 2025] [Originally Added On: November 2nd, 2012]
- 0026) Andropause: A Diagnosis Whose Time Has Come [Last Updated On: June 3rd, 2025] [Originally Added On: November 16th, 2012]
- 0027) Dealing With Mood Disorders During the Holidays (Depression, Anxiety, Depersonalization) - Video [Last Updated On: February 7th, 2025] [Originally Added On: November 26th, 2012]
- 0028) Testosterone Roundtable -- Hypergonadism and Testosterone Replacement Therapy (Part 6) - Video [Last Updated On: February 19th, 2025] [Originally Added On: December 10th, 2012]
- 0029) Battling my Testosterone Replacement Therapy Doctor, Carpal Tunnel Syndrome, and Weightlifting - Video [Last Updated On: March 12th, 2013] [Originally Added On: March 12th, 2013]
- 0030) Low T? Testosterone Replacement Therapy - Video [Last Updated On: March 13th, 2013] [Originally Added On: March 13th, 2013]
- 0031) Testosterone Replacement Therapy: Nothing To Be Ashamed Of: Strike First Nutrition - Video [Last Updated On: May 18th, 2013] [Originally Added On: May 18th, 2013]
- 0032) Testosterone Replacement Therapy: Symptoms of Low Testosterone - Strike First Nutrition - Video [Last Updated On: May 18th, 2013] [Originally Added On: May 18th, 2013]
- 0033) Testosterone Replacement Therapy Testimonial - Video [Last Updated On: June 15th, 2013] [Originally Added On: June 15th, 2013]
- 0034) Taurus Male Clinic Testosterone Replacement Therapy - Video [Last Updated On: July 28th, 2013] [Originally Added On: July 28th, 2013]
- 0035) Can I Quit TRT Or Testosterone Replacement Therapy? By Low Testosterone Expert Dr David Asher - Video [Last Updated On: March 16th, 2017] [Originally Added On: August 7th, 2013]
- 0036) What Are The Side Effects of TRT Testosterone Replacement Therapy? By Low T Expert Dr. David Asher - Video [Last Updated On: August 7th, 2013] [Originally Added On: August 7th, 2013]
- 0037) Bill Jones 1513 Testosterone Replacement Therapy Testimonial - Video [Last Updated On: August 8th, 2013] [Originally Added On: August 8th, 2013]
- 0038) 2013-08-06 Testosterone Replacement Therapy - Video [Last Updated On: August 10th, 2013] [Originally Added On: August 10th, 2013]
- 0039) Testosterone Replacement Therapy West Palm Beach Florida - Video [Last Updated On: August 18th, 2013] [Originally Added On: August 18th, 2013]
- 0040) Testosterone Replacement Therapy Testimony from Patient of Body Renew Medical in Lees Summit MO - Video [Last Updated On: September 2nd, 2013] [Originally Added On: September 2nd, 2013]
- 0041) FGSW - An Update On My Testosterone Replacement Therapy: Doctor's Visit 09.16.13 - Video [Last Updated On: September 19th, 2013] [Originally Added On: September 19th, 2013]
- 0042) Testosterone Replacement Therapy - Testosterone Treatment [Last Updated On: March 25th, 2025] [Originally Added On: October 31st, 2013]
- 0043) Testosterone Side Effects from Testosterone Replacement Therapy [Last Updated On: January 11th, 2018] [Originally Added On: November 3rd, 2013]
- 0044) FGSW - An Update On My Testosterone Replacement Therapy (TRT) 11.08.13: Getting No Sleep! - Video [Last Updated On: November 14th, 2013] [Originally Added On: November 14th, 2013]
- 0045) WebMD: Erectile Dysfunction: Testosterone Replacement Therapy [Last Updated On: January 17th, 2026] [Originally Added On: November 25th, 2013]
- 0046) Testosterone Replacement Therapy! Male Hormones! [Last Updated On: January 15th, 2018] [Originally Added On: November 25th, 2013]
- 0047) FGSW - Testosterone Replacement Therapy TRT Update: Am I Back Where I Started - 11.25.13 - Video [Last Updated On: November 27th, 2013] [Originally Added On: November 27th, 2013]
- 0048) Testosterone replacement therapy can carry health risks - CBS News [Last Updated On: January 16th, 2018] [Originally Added On: December 8th, 2013]
- 0049) Reclaim Your Energy and Sex Drive | Testosterone Replacement ... [Last Updated On: April 6th, 2025] [Originally Added On: December 21st, 2013]
- 0050) Low Testosterone Therapy and Treatment - Do You Have Low ... [Last Updated On: November 25th, 2025] [Originally Added On: December 24th, 2013]
- 0051) How Long Does it Take for Testosterone Replacement Therapy to ... [Last Updated On: December 30th, 2017] [Originally Added On: January 3rd, 2014]
- 0052) Testosterone Therapy - Bioidentical Testosterone Replacement [Last Updated On: January 23rd, 2018] [Originally Added On: January 9th, 2014]
- 0053) Transdermal testosterone replacement therapy - Video abstract 43475 - Video [Last Updated On: January 11th, 2014] [Originally Added On: January 11th, 2014]
- 0054) Testosterone Therapy - Bioidentical Testosterone Replacement ... [Last Updated On: December 21st, 2017] [Originally Added On: January 13th, 2014]
- 0055) Testosterone Side Effects from Testosterone Replacement ... [Last Updated On: January 30th, 2026] [Originally Added On: January 20th, 2014]
- 0056) MyAntiAgingMD The Leader In Testosterone Replacement Therapy - Video [Last Updated On: October 21st, 2020] [Originally Added On: January 29th, 2014]
- 0057) The benefits and risks of testosterone replacement therapy ... [Last Updated On: October 15th, 2020] [Originally Added On: February 6th, 2014]
- 0058) The Secret Female Hormone: How Testosterone Replacement Can Change Your Life [Last Updated On: October 28th, 2020] [Originally Added On: February 11th, 2014]
- 0059) Testosterone Replacement Therapy found to be linked to Heart Problems [Last Updated On: April 19th, 2025] [Originally Added On: February 25th, 2014]
- 0060) Serious Side Effects Linked to Testosterone Therapy [Last Updated On: September 17th, 2025] [Originally Added On: February 27th, 2014]
- 0061) Doctor Reveals How Getting off Testosterone Will Hurt Fighters on It [Last Updated On: November 27th, 2020] [Originally Added On: March 4th, 2014]
- 0062) California joins Nevada in banning testosterone replacement therapy [Last Updated On: October 4th, 2020] [Originally Added On: March 6th, 2014]
- 0063) Testosterone Replacement Therapy: How to Administer Expert TRT By John K. Crisler, DO - Video [Last Updated On: October 31st, 2020] [Originally Added On: March 9th, 2014]
- 0064) FGSW - Week 14 Weigh-In & Update: Going Back To The Endocrinologist - Video [Last Updated On: March 29th, 2014] [Originally Added On: March 29th, 2014]
- 0065) Drug Recall Attorney at Herrera Law Firm, Inc., Comments on Reported Link Between Testosterone Drugs and Heart Attack ... [Last Updated On: November 30th, 2020] [Originally Added On: April 2nd, 2014]
- 0066) FGSW - Testosterone Replacement Therapy Update 03.27.14: An Improvement?? - Video [Last Updated On: October 8th, 2020] [Originally Added On: April 2nd, 2014]
- 0067) FGSW Weekly Weigh In & Update 15 Still Working On Mobility 03 31 14 - Video [Last Updated On: October 15th, 2020] [Originally Added On: April 5th, 2014]
- 0068) Discover the risk of prostate cancer with testosterone replacement therapy - Video [Last Updated On: October 1st, 2020] [Originally Added On: April 5th, 2014]
- 0069) FGSW - Weekly Weigh In & Update 15: Still Working On Mobility 03.31.14 - Video [Last Updated On: October 3rd, 2020] [Originally Added On: April 7th, 2014]
- 0070) Testosterone Replacement Therapy - Video [Last Updated On: October 1st, 2020] [Originally Added On: April 12th, 2014]
- 0071) Reclaim Your Energy and Sex Drive | Testosterone ... [Last Updated On: April 21st, 2025] [Originally Added On: April 14th, 2014]
- 0072) Low Testosterone Claims: Options in a Growing Class Action Suit - Video [Last Updated On: November 25th, 2020] [Originally Added On: April 26th, 2014]
- 0073) Acrux falls 15% on sales warning [Last Updated On: September 28th, 2025] [Originally Added On: April 28th, 2014]
- 0074) Testosterone Replacement Therapy in Men - myVMC [Last Updated On: November 1st, 2020] [Originally Added On: April 30th, 2014]
- 0075) NJ-Based Law Firm Exploring Potential Legal Claims from Side Effects of Testosterone Replacement Therapy [Last Updated On: October 22nd, 2020] [Originally Added On: May 1st, 2014]
- 0076) Viewer Mail - Testosterone Replacement Therapy/TRT Not Natty, Balls Busted, etc. - Video [Last Updated On: October 2nd, 2020] [Originally Added On: May 4th, 2014]
- 0077) Seen At 11: Experts Urge Caution When Using Popular Hormone Replacement Therapy [Last Updated On: November 11th, 2020] [Originally Added On: May 10th, 2014]
- 0078) Are Low-T Drugs Putting Patients At High Risk? [Last Updated On: October 15th, 2020] [Originally Added On: May 10th, 2014]
- 0079) Seen At 11: Testosterone Replacement Therapy Could Come With Serious Side Effects - Video [Last Updated On: May 11th, 2014] [Originally Added On: May 11th, 2014]
- 0080) 1513 Hormone Replacement Therapy for Men - Video [Last Updated On: October 15th, 2020] [Originally Added On: June 13th, 2014]
Word Count: 1138