Video Link: https://vimeo.com/290597923
Video Download: Click Here To Download Video
Video Stream: Click Here To Stream Video
Unless you have been imitating Rip Van Winkle for several years, you are aware that Testosterone Replacement Therapy (TRT) has exploded in the last decade.
However, there have been very few studies that have examined the long-term effects of taking testosterone on cardiovascular health and other vital functions concerning the health effects on men receiving the treatment.
 But that has changed.
But that has changed.
Recently, investigators from Brigham and Women's Hospital (BWH) report the results of Testosterone's Effects on Atherosclerosis Progression in Aging Men (TEAAM) trial in the Journal of the American Medical Association (JAMA).
The three-year study finds that testosterone administration had no effect on the progression of hardening of the arteries in older men with low to low-normal testosterone levels and did not significantly improve sexual function or health-related quality of life.
Shehzad Basaria, M.B.B.S., MD, from Harvard Medical School in Boston, and colleagues studied the effect of testosterone administration on atherosclerosis progression in older men.
Three hundred eight men aged 60 years or older (patients had a mean age of 67.6 years), with low or low-normal testosterone levels, volunteered and were treated with up to 7.5 g of 1 percent testosterone (156 men) or placebo gel packets (152 men) daily for three years.
In testosterone-treated patients, doses were adjusted periodically to achieve testosterone levels between 500 and 900 ng/dL.
Additionally, 42% of participants had hypertension, 15% had diabetes, 15% had cardiovascular disease, and 27% were obese.
The researchers assessed sexual function using the International Index of Erectile Function, a validated 15-item questionnaire that assesses five domains of sexual function (erectile function, orgasmic function, sexual desire, intercourse satisfaction, and overall sexual satisfaction).
They used the Medical Outcomes Study 36-item short-form health survey (SF-36) to assess health-related QOL.
"The results of this trial suggest that testosterone should not be used indiscriminately by men," said Dr. Bhasin, director of BWH's Research Program in Men's Health: Aging and Metabolism and director of the Boston Claude D. Pepper Older Americans Independence Center at BWH.
He added that "We find that men with low and low-normal testosterone are unlikely to derive benefits regarding sexual function or quality of life -- two reasons why men may seek testosterone therapy.
And although we find that testosterone did not affect the rate of hardening of the arteries, we need long-term data from large trials to determine testosterone's effects on other major cardiovascular events."
No Significant Difference
The researchers also observed no significant difference in the rate of change in intima-media thickness (a measurement of the thickness of the innermost two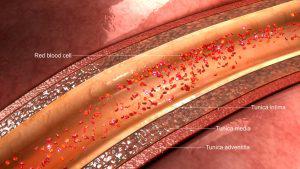 layers of the wall of an artery...0.010 mm/year in the placebo group versus 0.012 mm/year in the testosterone group; P = 0.89) or in the rate of change in the coronary artery calcium score, which is a cardiac CT scan for coronary calcium in a non-invasive way of measuring calcified plaque in the coronary arteries — the vessels that supply oxygen-containing blood to the heart muscle...(41.4 versus 31.4 Agatston units/year; P = 0.54).
layers of the wall of an artery...0.010 mm/year in the placebo group versus 0.012 mm/year in the testosterone group; P = 0.89) or in the rate of change in the coronary artery calcium score, which is a cardiac CT scan for coronary calcium in a non-invasive way of measuring calcified plaque in the coronary arteries — the vessels that supply oxygen-containing blood to the heart muscle...(41.4 versus 31.4 Agatston units/year; P = 0.54).
In the individuals assigned to receive testosterone, changes in intima-media thickness or calcium scores had no link with a difference in testosterone levels.
There was no significant difference between-group sexual drive, erectile dysfunction, sexual function ability, partner intimacy, or health-related quality of life.
"Our research shows convincingly that testosterone therapy does not affect the rate of atherosclerosis progression, but we need much larger, randomized trials to determine if testosterone treatment impacts heart attack and stroke risk," Bhasin told MedPage Today.
He added that if this is the case, the mechanism does not appear to be through the treatment's impact on atherogenesis.
"Testosterone may be affecting some other mechanism, such as plaque stability or clotting within the blood vessel," he said.
"Because this trial was only powered to evaluate atherosclerosis progression, these findings should not be interpreted as establishing the cardiovascular safety of testosterone use in older men," the authors write.
"Our study has important implications for clinical practice, and for older men who are seeking testosterone therapy," said Bhasin.
"Many men, as they age, experience a decline in testosterone and sexual function and vitality.
But our study finds that taking testosterone, when levels are in the low to the low-normal range, may not improve sexual function or quality of life."
The study was supported by Solvay Pharmaceuticals/Abbvie Pharmaceuticals, which provided testosterone and placebo gel.
 Testosterone, a hormone primarily secreted by the testicles, plays a vital role not only in male reproductive tissues but also in muscle growth, bone mass, and body hair.
Testosterone, a hormone primarily secreted by the testicles, plays a vital role not only in male reproductive tissues but also in muscle growth, bone mass, and body hair.
As men get older, their testosterone levels naturally decline -- on average by 1 percent a year after age 40.
Previous studies that have aimed to examine rates of cardiovascular events in men taking testosterone have reported conflicting results but have raised concerns that testosterone therapy might increase a person's risk of a heart attack or stroke.
Atherosclerosis, or the buildup of plaque in the arteries, is a critical risk factor for such cardiovascular events.
But Cardiovascular Safety for TRT Remains an Open Question
While earlier studies examining the impact of TRT on cardiovascular disease (CVD) risk in older men have been mixed, the TEAAM trial was not powered to weigh in on testosterone's effect on CVD events in this population, the researchers warned.
As a result, the findings should not be interpreted as establishing the treatment's safety in older men, they emphasized.
The TEAAM trial was designed to examine atherosclerosis progression and not cardiovascular events — further studies will be needed to determine the cardiovascular safety of testosterone use in older men.
The research team also notes that comparing patients using statins to those who are not could be another important direction for future studies.
Baseline characteristics among the treatment and placebo groups were similar: mean patient age at randomization was 67.6 years, 42% of participants had hypertension, 15% had diabetes, 15% had cardiovascular disease, and 27% were obese.
The authors reported that the rate of change in the CAC score was 41.4 Agatston units/year in the placebo group and 31.4 Agatston units/year in the testosterone group for an adjusted mean difference of 10.8 Agatston units/year (95% CI 45.7 to 24.2, P=0.54).
Study limitations included the high rate of loss to follow-up and the fact that the effectiveness of participant blinding was not assessed.
Bhasin said the failure to show a positive impact on these secondary endpoints has significant implications for the use of TRT in relatively healthy middle-aged and older men.
He said the dramatic rise in TRT use among relatively healthy, aging men with borderline low testosterone levels over the last decade had been primarily driven by the desire to improve sexual function and QOL.
driven by the desire to improve sexual function and QOL.
"Testosterone is being used indiscriminately, and it shouldn't be," he said.
"Many middle-aged and older men are seeking this treatment to address sexual symptoms or to improve their quality of life. Our study clearly showed that the treatment has little impact in men whose testosterone levels are near normal."
He noted that although several large, randomized trials evaluating TRT in older men are nearing completion, including the NIH's Trial, they are not designed to determine CVD risk.
"We need a TRT test with cardiovascular event rate as the primary outcome, and it needs to happen fairly quickly," he said.
Reference
Testosterone Treatment and Coronary Artery Plaque Volume in Older Men With Low Testosterone.
Contact Us Today For A Free Consultation

- 0001) Adverse Effects of Testosterone Therapy in Adult Men: A Systematic Review and Meta-Analysis [Last Updated On: July 2nd, 2024] [Originally Added On: June 4th, 2010]
- 0002) Low Testosterone Levels, Foods That Increase Testosterone Levels wwwSelf-Improvement-Bible.com [Last Updated On: November 12th, 2023] [Originally Added On: May 30th, 2011]
- 0003) Low Testosterone in Men: The Next Big Thing in Medicine! - Abraham Morgentaler, MD [Last Updated On: May 7th, 2023] [Originally Added On: June 3rd, 2011]
- 0004) How To Determine Testosterone Levels By Looking At Your Ring Finger [Last Updated On: January 28th, 2026] [Originally Added On: June 30th, 2011]
- 0005) Prolab Horny Goat Weed Testosterone Booster Supplement Review [Last Updated On: November 23rd, 2023] [Originally Added On: July 19th, 2011]
- 0006) The Healthy Skeptic: Products make testosterone claims [Last Updated On: August 13th, 2024] [Originally Added On: September 11th, 2011]
- 0007) How To Naturally Increase Testosterone [Last Updated On: November 21st, 2023] [Originally Added On: September 28th, 2011]
- 0008) Testosterone Production - Video [Last Updated On: November 25th, 2024] [Originally Added On: November 20th, 2011]
- 0009) Testosterone makes us less cooperative and more egocentric, study finds [Last Updated On: January 23rd, 2018] [Originally Added On: February 1st, 2012]
- 0010) Testosterone makes us less cooperative and more egocentric [Last Updated On: January 24th, 2018] [Originally Added On: February 1st, 2012]
- 0011) Too much testosterone makes for bad decisions, tests show [Last Updated On: April 30th, 2025] [Originally Added On: February 1st, 2012]
- 0012) Today in Research: Testosterone's Negative Effects; Diet Soda Death [Last Updated On: January 2nd, 2018] [Originally Added On: February 2nd, 2012]
- 0013) Testosterone drives ego, trips cooperation [Last Updated On: December 25th, 2025] [Originally Added On: February 4th, 2012]
- 0014) FDA approves BioSante/Teva's testosterone gel [Last Updated On: April 28th, 2025] [Originally Added On: February 15th, 2012]
- 0015) 'Manly' Fingers Make For Strong Jawline in Young Boys [Last Updated On: December 14th, 2025] [Originally Added On: February 15th, 2012]
- 0016) Teva, BioSante Win U.S. Approval for Testosterone Therapy [Last Updated On: February 10th, 2026] [Originally Added On: February 15th, 2012]
- 0017) BioSante Gains on Approval of Testosterone Gel: Chicago Mover [Last Updated On: January 8th, 2018] [Originally Added On: February 16th, 2012]
- 0018) BioSante soars following drug approval from FDA [Last Updated On: December 26th, 2017] [Originally Added On: February 16th, 2012]
- 0019) Antibodies, Not Hard Bodies: The Real Reason Women Drool Over Brad Pitt [Last Updated On: December 24th, 2017] [Originally Added On: February 21st, 2012]
- 0020) Almark Publishing Releases Book From Mark Rosenberg, M.D. Revealing Natural Discoveries Associated With Low ... [Last Updated On: May 3rd, 2025] [Originally Added On: February 28th, 2012]
- 0021) Testosterone Replacement Clinic Comes to Kansas City with Potential to Help Thousands of Men [Last Updated On: May 2nd, 2025] [Originally Added On: March 1st, 2012]
- 0022) Study examines the relative roles of testosterone and its metabolite, dihydrotestosterone in men [Last Updated On: December 23rd, 2025] [Originally Added On: March 7th, 2012]
- 0023) The Role of 5{alpha}-Reductase Inhibition in Men Receiving Testosterone Replacement Therapy [Editorial] [Last Updated On: December 21st, 2017] [Originally Added On: March 7th, 2012]
- 0024) Effect of Testosterone Supplementation With and Without a Dual 5{alpha}-Reductase Inhibitor on Fat-Free Mass in Men ... [Last Updated On: January 3rd, 2018] [Originally Added On: March 7th, 2012]
- 0025) Why We Like Men Who Can Keep Their Cool [Last Updated On: December 30th, 2017] [Originally Added On: March 7th, 2012]
- 0026) Testosterone And Heart Health [Last Updated On: May 1st, 2025] [Originally Added On: March 10th, 2012]
- 0027) Your Life on Testosterone: Overly Sure of Yourself, Unwilling to Listen [Last Updated On: November 25th, 2018] [Originally Added On: March 15th, 2012]
- 0028) Mayo Clinic-TGen study role testosterone may play in triple negative breast cancer [Last Updated On: February 1st, 2026] [Originally Added On: March 23rd, 2012]
- 0029) A dose of testosterone might not cure what ails you [Last Updated On: January 23rd, 2018] [Originally Added On: March 25th, 2012]
- 0030) Green tea could aid athletes hide testosterone doping [Last Updated On: March 16th, 2026] [Originally Added On: March 25th, 2012]
- 0031) TGen Study Role Testosterone May Play in Triple Negative Breast Cancer [Last Updated On: January 19th, 2026] [Originally Added On: March 26th, 2012]
- 0032) Testosterone low, but responsive to competition, in Amazonian tribe [Last Updated On: January 23rd, 2018] [Originally Added On: March 28th, 2012]
- 0033) Competition-linked bursts of testosterone are fundamental aspect of human biology, study of Amazonian tribe suggests [Last Updated On: December 25th, 2017] [Originally Added On: March 28th, 2012]
- 0034) Playing football boosts testosterone levels by 30 percent! [Last Updated On: February 4th, 2024] [Originally Added On: March 28th, 2012]
- 0035) Testosterone low, but responsive to competition, in Amazonian tribe -- with slideshow [Last Updated On: February 3rd, 2026] [Originally Added On: March 28th, 2012]
- 0036) The benefits of testosterone pellet therapy [Last Updated On: January 24th, 2018] [Originally Added On: March 29th, 2012]
- 0037) Low testosterone levels cause health woes [Last Updated On: November 25th, 2018] [Originally Added On: March 30th, 2012]
- 0038) Heart Failure Patients Getting Relief from Testosterone Supplements [Last Updated On: May 5th, 2025] [Originally Added On: April 21st, 2012]
- 0039) Study Finds Fatherhood Suppresses Testosterone [Last Updated On: May 4th, 2025] [Originally Added On: May 3rd, 2012]
- 0040) Low testosterone levels could raise diabetes risk for men [Last Updated On: January 26th, 2018] [Originally Added On: May 5th, 2012]
- 0041) Why low testosterone may increase your risk of diabetes [Last Updated On: November 25th, 2024] [Originally Added On: May 5th, 2012]
- 0042) Diabetes link to low testosterone [Last Updated On: November 25th, 2024] [Originally Added On: May 5th, 2012]
- 0043) Testosterone Linked to Weight Loss in Obese Men [Last Updated On: January 2nd, 2018] [Originally Added On: May 11th, 2012]
- 0044) Testosterone may help weight loss [Last Updated On: November 25th, 2024] [Originally Added On: May 11th, 2012]
- 0045) Testosterone-fuelled infantile males might be a product of Mom's behaviour [Last Updated On: December 25th, 2017] [Originally Added On: May 11th, 2012]
- 0046) Testosterone-fueled infantile males might be a product of Mom's behavior [Last Updated On: January 6th, 2018] [Originally Added On: May 11th, 2012]
- 0047) Testosterone supplements may help obese men lose weight [Last Updated On: January 5th, 2018] [Originally Added On: May 11th, 2012]
- 0048) Testosterone supplements 'can help men lose their middle-aged spread' [Last Updated On: November 25th, 2024] [Originally Added On: May 12th, 2012]
- 0049) Some doctors question safety of testosterone replacement therapy [Last Updated On: January 20th, 2018] [Originally Added On: May 15th, 2012]
- 0050) Health Canada Approves New Testosterone Topical Solution for Men [Last Updated On: May 15th, 2025] [Originally Added On: May 15th, 2012]
- 0051) Environment trumps genes in testosterone levels, study finds [Last Updated On: May 8th, 2025] [Originally Added On: May 15th, 2012]
- 0052) Global Testosterone Replacement Therapy (TRT) Industry [Last Updated On: May 7th, 2025] [Originally Added On: May 21st, 2012]
- 0053) Testosterone Fuels Boom, Swindler Sows Panic: Top Business Books [Last Updated On: January 13th, 2018] [Originally Added On: June 2nd, 2012]
- 0054) Increase in testosterone drug use [Last Updated On: April 12th, 2018] [Originally Added On: June 4th, 2012]
- 0055) Testosterone Promotes Agression Automatically [Last Updated On: January 29th, 2018] [Originally Added On: June 9th, 2012]
- 0056) Testosterone shown to help sexually frustrated women [Last Updated On: January 27th, 2018] [Originally Added On: June 9th, 2012]
- 0057) Research and Markets: Testosterone Replacement Therapy (TRT) - Global Strategic Business Report [Last Updated On: December 23rd, 2017] [Originally Added On: June 12th, 2012]
- 0058) Proposed testosterone testing of some female olympians challenged by Stanford scientists [Last Updated On: January 30th, 2018] [Originally Added On: June 14th, 2012]
- 0059) Testosterone Makes Bosses Into Jerks, Says Paul Zak [Last Updated On: January 8th, 2018] [Originally Added On: June 14th, 2012]
- 0060) Testosterone Therapy: A Misguided Approach to Erectile Dysfunction (ED) [Last Updated On: May 10th, 2025] [Originally Added On: June 20th, 2012]
- 0061) New drugs, new ways to target androgens in prostate cancer therapy [Last Updated On: January 8th, 2018] [Originally Added On: June 20th, 2012]
- 0062) Long-term testosterone treatment for men results in reduced weight and waist size [Last Updated On: January 19th, 2018] [Originally Added On: June 23rd, 2012]
- 0063) Declining testosterone levels in men not part of normal aging, study finds [Last Updated On: December 27th, 2017] [Originally Added On: June 23rd, 2012]
- 0064) Low testosterone not normal part of aging [Last Updated On: December 22nd, 2017] [Originally Added On: June 25th, 2012]
- 0065) Testosterone Does Not Necessarily Wane With Age [Last Updated On: January 16th, 2026] [Originally Added On: June 25th, 2012]
- 0066) Overweight men can boost low testosterone levels by losing weight [Last Updated On: February 8th, 2026] [Originally Added On: June 25th, 2012]
- 0067) Testosterone-replacement therapy improves symptoms of metabolic syndrome [Last Updated On: January 14th, 2018] [Originally Added On: June 26th, 2012]
- 0068) Testosterone therapy takes off pounds [Last Updated On: February 14th, 2026] [Originally Added On: June 26th, 2012]
- 0069) Weight loss may boost men's testosterone [Last Updated On: May 9th, 2025] [Originally Added On: June 27th, 2012]
- 0070) Low Testosterone? Study finds age may not be to blame [Last Updated On: May 12th, 2025] [Originally Added On: July 1st, 2012]
- 0071) Do you have low testosterone? [Last Updated On: March 5th, 2026] [Originally Added On: July 8th, 2012]
- 0072) Wall Streeters Buying Testosterone for an Edge [Last Updated On: May 11th, 2025] [Originally Added On: July 12th, 2012]
- 0073) Beefy Wall Street Traders rub on testosterone [Last Updated On: February 20th, 2024] [Originally Added On: July 12th, 2012]
- 0074) Tale of two runners exposes flawed Olympic thinking [Last Updated On: December 23rd, 2024] [Originally Added On: July 19th, 2012]
- 0075) Genetic markers for testosterone and estrogen level regulation identified [Last Updated On: January 6th, 2018] [Originally Added On: July 20th, 2012]
- 0076) BUSM researchers identify genetic markers for testosterone, estrogen level regulation [Last Updated On: December 18th, 2017] [Originally Added On: July 20th, 2012]
- 0077) DRS. OZ AND ROIZEN: How to reap the benefits of normal testosterone levels [Last Updated On: December 23rd, 2024] [Originally Added On: July 21st, 2012]
- 0078) How Testosterone Drives History [Last Updated On: December 24th, 2024] [Originally Added On: July 22nd, 2012]
- 0079) Testosterone replacement is "fountain of youth" for men [Last Updated On: January 3rd, 2018] [Originally Added On: July 27th, 2012]
- 0080) Pill for low testosterone in men heads for phase II clinical trials [Last Updated On: December 31st, 2017] [Originally Added On: August 2nd, 2012]
Word Count: 1204